What happened?:
On January 24th, at approximately 13:30, two service provider personnel (an inspection team leader and assistant) were performing loose lifting gear inspections on and around the riser deck area of a drillship in the US Gulf of Mexico. The task was visually
inspecting slings, recording serial numbers and applying the current colour code.
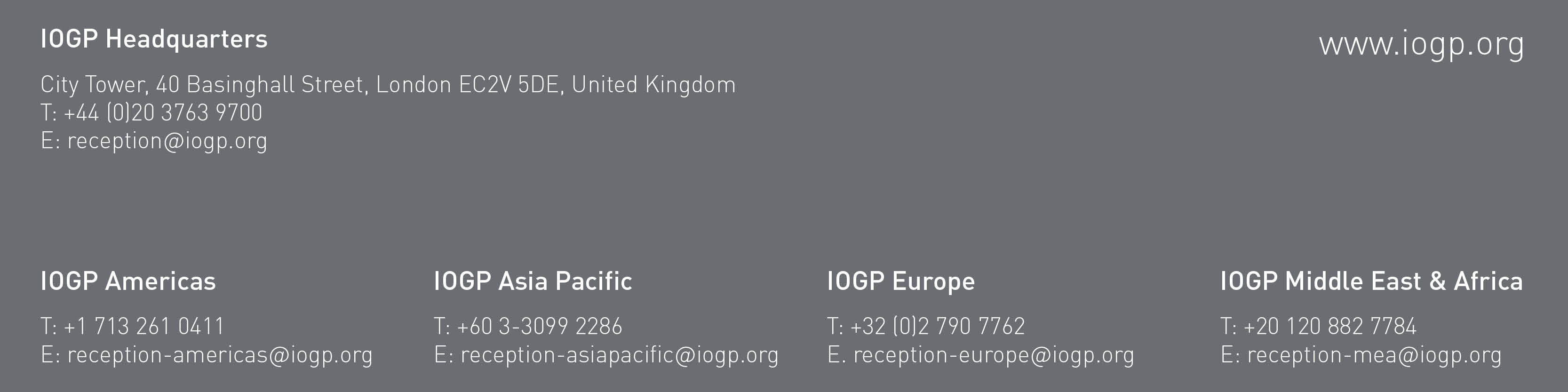
During the inspection, the inspection team leader observed two slings rigged up to a load of 5 metal plates which were stacked vertically, resting on dunnage, and secured to a stanchion by a single 2 ratchet strap (see Figure 1). The slings had been left
in place on the plates after they were landed by the crane for efficiency and ease of relocation when needed.
The plates were all 4 x 8 feet; three were 3/8 thickness and the other two were 1 thickness (see Figure 2).
The plates were onboard for deck strengthening as some configurations of well test equipment require deck strengthening for safe operation.
The inspection team leader attempted to, and was successful in, sliding one of the slings from the plates on the inboard side (#1 represented above in Figure #1), but he discovered the second sling (#2 represented above in Figure #1) was pinched between
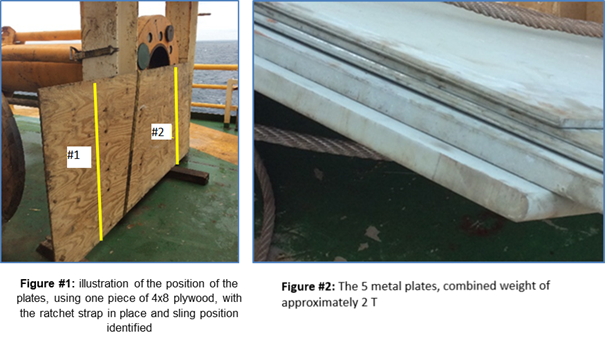
the rear of the plates and the stanchion, preventing it from being taken off on the outboard side. He then called his assistant and requested that he loosen the ratchet strap, presumably to allow for movement of the plates for the pinched sling to be removed
for inspection.
The inspection team leader then leaned his back against the plates; The reason for this is unknown, but it is assumed the intention was to support the plates in their standing position when the ratchet strap was loosened. When he was standing in this position,
directly in front of him was a framework for the drilling bail rack. When the ratchet strap was manipulated by the assistant, the hook (rachet strap) released, (see Figure #3), allowing the plates to free fall forward (away from the stanchion) under their
own weight, fatally trapping the inspection team leader between the plates and the framework of the drilling bail rack (see Figure #4).
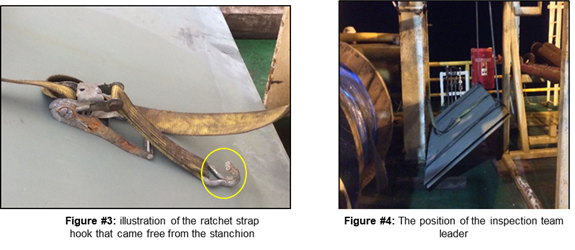
The weight of the falling metal plates, overwhelmed the lead inspector, who was caught in the line of fire and pinned between the plates and the solid frame.
First responders arrived at the scene and attempted to manually remove the plates but were unable to due to their weight.
|